Nerve injuries occur in about 40% of type III ( Gartlands classification) supracondylar fractures. 
 Treatment. Extension type injuries are more common (80-95%) than flexion type. Aims: We aimed to identify the pattern of nerve injury associated with paediatric supracondylar fractures of the humerus.
Treatment. Extension type injuries are more common (80-95%) than flexion type. Aims: We aimed to identify the pattern of nerve injury associated with paediatric supracondylar fractures of the humerus.  Clinical examination for elbow flexion, extension, range of motion and carrying angle were performed, followed by ultrasonographic examination to determine position of the ulnar nerve in relation to the medial epicondyle upon elbow flexion and extension. The mean age was 6.0 years, ranging from 1 to 12 years. 4% (72/2051) 5. 4% (88/2051) 4. Radial nerve palsy, in addition to ulnar nerve injury, has also been described during open reduction and pinning of supracondylar fractures (Brown and Zinar 1995). The relative incidence of nerve injuries after supracondylar humerus fractures is reported with 1220% due to traumatic tenting or entrapment and with 26.5% iatrogenic lesions during closed reposition or percutaneous pinning . depending on the fracture pattern and associated injuries (i.e., nerve injury or open fracture).
Clinical examination for elbow flexion, extension, range of motion and carrying angle were performed, followed by ultrasonographic examination to determine position of the ulnar nerve in relation to the medial epicondyle upon elbow flexion and extension. The mean age was 6.0 years, ranging from 1 to 12 years. 4% (72/2051) 5. 4% (88/2051) 4. Radial nerve palsy, in addition to ulnar nerve injury, has also been described during open reduction and pinning of supracondylar fractures (Brown and Zinar 1995). The relative incidence of nerve injuries after supracondylar humerus fractures is reported with 1220% due to traumatic tenting or entrapment and with 26.5% iatrogenic lesions during closed reposition or percutaneous pinning . depending on the fracture pattern and associated injuries (i.e., nerve injury or open fracture). 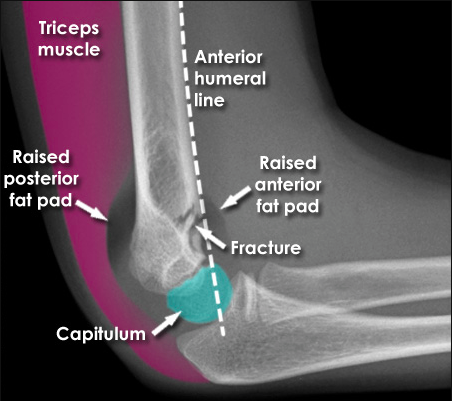 surgical approach necessary for fracture fixation should first be. A review of the literature reports iatrogenic ulnar nerve injury at a As the fracture or dislocation itself is a painful and distressing injury, the presence of a nerve injury may not be recognised immediately. Supracondylar humeral fracture (SHF) is considered the second most common fracture (after distal radius fracture) in childhood, accounting for approximately 15% of all pediatric fractures . Gross deformity, swelling, bruising. When this occurs, the olecranon acts as a fulcrum after engaging in the olecranon fossa. What is supracondylar humerus fracture? A supracondylar humerus fracture is defined as a fracture of the lower end (distal part) of the humerus just above the elbow joint. This fracture pattern is comparatively less common in adults but is the most frequent sort of elbow fracture in children.
surgical approach necessary for fracture fixation should first be. A review of the literature reports iatrogenic ulnar nerve injury at a As the fracture or dislocation itself is a painful and distressing injury, the presence of a nerve injury may not be recognised immediately. Supracondylar humeral fracture (SHF) is considered the second most common fracture (after distal radius fracture) in childhood, accounting for approximately 15% of all pediatric fractures . Gross deformity, swelling, bruising. When this occurs, the olecranon acts as a fulcrum after engaging in the olecranon fossa. What is supracondylar humerus fracture? A supracondylar humerus fracture is defined as a fracture of the lower end (distal part) of the humerus just above the elbow joint. This fracture pattern is comparatively less common in adults but is the most frequent sort of elbow fracture in children.  Of all complications associated with supracondylar fractures, nerve injury ranks highest, although reports of the incidence of specific neurapraxia vary. In the literature, the most common neurologic deficit associated with ScHF in children is reported to be neurapraxia which usually resolves spontaneously within two to three Results. Guidelines.
Of all complications associated with supracondylar fractures, nerve injury ranks highest, although reports of the incidence of specific neurapraxia vary. In the literature, the most common neurologic deficit associated with ScHF in children is reported to be neurapraxia which usually resolves spontaneously within two to three Results. Guidelines.  Ulnar nerve is prone to injury following flexion type of supracondylar fractures and loss of sensation in its distribution can be examined following weakness of intrinsic muscles of the hand. Ipsilateral supracondylar humerus and forearm/wrist fractures warrant timely pinning of both fractures to decrease risk of compartment syndrome. These fractures affect the distal humerus. Supracondylar fractures of the humerus in children are common and can be distressing injuries to the child, the parents and to the surgical team. A supracondylar humerus fracture is a fracture of the distal humerus just above the elbow joint. There were 182 boys (67%) and 90 girls (33%). Isolated supracondylar fractures are extraarticular, lying beyond the proximal extensions of the joint capsule. Non-displaced fracture may have limited swelling, but child will refuse to move arm. In 10 (90.1%) of these 11 cases, nerve functions recovered completely (excellent outcome) and in one (9.9%) case partial recovery was seen (good outcome). Lateral displacement of the fracture fragment may cause radial nerve damage resulting in failure to extend the wrist, supinate, or extend the thumb. Contents. The anterior interosseous nerve is most commonly affected by the initial injury, however ulnar nerve palsy is the most common post-operative complication.
Ulnar nerve is prone to injury following flexion type of supracondylar fractures and loss of sensation in its distribution can be examined following weakness of intrinsic muscles of the hand. Ipsilateral supracondylar humerus and forearm/wrist fractures warrant timely pinning of both fractures to decrease risk of compartment syndrome. These fractures affect the distal humerus. Supracondylar fractures of the humerus in children are common and can be distressing injuries to the child, the parents and to the surgical team. A supracondylar humerus fracture is a fracture of the distal humerus just above the elbow joint. There were 182 boys (67%) and 90 girls (33%). Isolated supracondylar fractures are extraarticular, lying beyond the proximal extensions of the joint capsule. Non-displaced fracture may have limited swelling, but child will refuse to move arm. In 10 (90.1%) of these 11 cases, nerve functions recovered completely (excellent outcome) and in one (9.9%) case partial recovery was seen (good outcome). Lateral displacement of the fracture fragment may cause radial nerve damage resulting in failure to extend the wrist, supinate, or extend the thumb. Contents. The anterior interosseous nerve is most commonly affected by the initial injury, however ulnar nerve palsy is the most common post-operative complication.  Pin migration (most common ~2%) Infection (1-2.4%), higher risk in <4.5 y/o. Vascular Injury classification. Methods: A questionnaire was designed for this study, which included the choice of pinning technique, methods of elbow motion, and perception on the restoration of elbow ROM. Some surgeons use lateral-only pins to avoid iatrogenic ulnar nerve injury. Of the 77 patients with supracondylar fractures of humerus recruited in the study, 46 (59.7%) were males. Patients and methods: Over a 17 year period, between 1996 and 2012, 166 children were referred to our specialist peripheral nerve injury unit. Supracondylar Humerus Fracture Protocol o Specific nerve and vascular exam imperative o AP & lateral radiographs imperative o Consider other injuries; distal radius fractures. Is There a Chance to Treat Modified Gartland Type IIB Pediatric Supracondylar Humerus Fractures With Closed Reduction and Casting? found the anterior interosseous nerve to be at highest risk in extension-type fractures.
Pin migration (most common ~2%) Infection (1-2.4%), higher risk in <4.5 y/o. Vascular Injury classification. Methods: A questionnaire was designed for this study, which included the choice of pinning technique, methods of elbow motion, and perception on the restoration of elbow ROM. Some surgeons use lateral-only pins to avoid iatrogenic ulnar nerve injury. Of the 77 patients with supracondylar fractures of humerus recruited in the study, 46 (59.7%) were males. Patients and methods: Over a 17 year period, between 1996 and 2012, 166 children were referred to our specialist peripheral nerve injury unit. Supracondylar Humerus Fracture Protocol o Specific nerve and vascular exam imperative o AP & lateral radiographs imperative o Consider other injuries; distal radius fractures. Is There a Chance to Treat Modified Gartland Type IIB Pediatric Supracondylar Humerus Fractures With Closed Reduction and Casting? found the anterior interosseous nerve to be at highest risk in extension-type fractures.  Inadvertent intra-articular hardware penetration. The incidence of vascular complications associated with supracondylar fractures ranges from 3.2 to 14.3% [5], nerve injuries are reported with a relative incidence of 1220% [6]. The rate of open reduction for fractures with a flexion-type injury pattern and for such fractures with and without ulnar nerve injury at presentation was assessed. Urgent. Although all upper limbs were affected, more than half 57 (74%) had the left upper limb affected and only 20 (26%) had their right upper limb affected.
Inadvertent intra-articular hardware penetration. The incidence of vascular complications associated with supracondylar fractures ranges from 3.2 to 14.3% [5], nerve injuries are reported with a relative incidence of 1220% [6]. The rate of open reduction for fractures with a flexion-type injury pattern and for such fractures with and without ulnar nerve injury at presentation was assessed. Urgent. Although all upper limbs were affected, more than half 57 (74%) had the left upper limb affected and only 20 (26%) had their right upper limb affected. 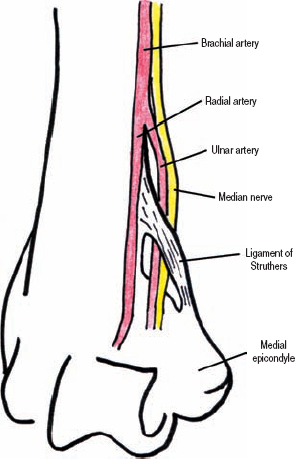 Once the x-ray happens, the injury is recordable, even if nothings broken or fractured and they go home an hour later. In the event they require an examination, and the doctor decides to keep them overnight for observation, then the incident is reportable . Avoiding nerve injury: there is always. Anterior Interosseous Nerve Palsy: This is the most commonly injured nerve in extension-type supracondylar fractures. Accurate and repetitive neuromuscular assessment is critical not just for medicolegal Injuries to the ulnar and radial nerves are less common. well as damage the median nerve, resulting inability to flex the wrist, or activate flexors of the thumb or digits. General: Physical Exam Elbow.
Once the x-ray happens, the injury is recordable, even if nothings broken or fractured and they go home an hour later. In the event they require an examination, and the doctor decides to keep them overnight for observation, then the incident is reportable . Avoiding nerve injury: there is always. Anterior Interosseous Nerve Palsy: This is the most commonly injured nerve in extension-type supracondylar fractures. Accurate and repetitive neuromuscular assessment is critical not just for medicolegal Injuries to the ulnar and radial nerves are less common. well as damage the median nerve, resulting inability to flex the wrist, or activate flexors of the thumb or digits. General: Physical Exam Elbow.  The most common mechanism of injury involves a fall on an outstretched hand Hand The hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. We report a case of Gartland type III supracondylar humeral fracture complicated by an entrapment of the median nerve following closed reduction and percutaneous pinning in a 5-year-old child. Epidemiology. prior to reduction and definitive fixation. Supracondylar fracture of the humerus median nerve. Radial Nerve Palsy: This has been found to be more common in Medial pins started too posteriorly on the medial epicondyle can affect the ulnar nerve, and again, lateral cortical penetration can be injurious to the radial nerve (Fig. Nerve injuries occuring after trauma It is recommended to immediately perform CMR (close manipulative reduction) in any case of supracondylar humeral fractures before transferring the patient to the operation room. This study involved evaluation of the elbows of 50 children between 4 to 14 years of age. distal fracture fragment will be angulated and/or displaced posteriorly.
The most common mechanism of injury involves a fall on an outstretched hand Hand The hand constitutes the distal part of the upper limb and provides the fine, precise movements needed in activities of daily living. We report a case of Gartland type III supracondylar humeral fracture complicated by an entrapment of the median nerve following closed reduction and percutaneous pinning in a 5-year-old child. Epidemiology. prior to reduction and definitive fixation. Supracondylar fracture of the humerus median nerve. Radial Nerve Palsy: This has been found to be more common in Medial pins started too posteriorly on the medial epicondyle can affect the ulnar nerve, and again, lateral cortical penetration can be injurious to the radial nerve (Fig. Nerve injuries occuring after trauma It is recommended to immediately perform CMR (close manipulative reduction) in any case of supracondylar humeral fractures before transferring the patient to the operation room. This study involved evaluation of the elbows of 50 children between 4 to 14 years of age. distal fracture fragment will be angulated and/or displaced posteriorly.  The ideal incision for the. The presence of an ulnar nerve injury at presentation resulted in an additional 6.7-fold higher risk of open reduction among flexion-type supracondylar humeral fractures. 1 Signs and symptoms.
The ideal incision for the. The presence of an ulnar nerve injury at presentation resulted in an additional 6.7-fold higher risk of open reduction among flexion-type supracondylar humeral fractures. 1 Signs and symptoms.  Earlier literature stated that radial nerve was the most commonly injured nerve in supracondylar fractures.
Earlier literature stated that radial nerve was the most commonly injured nerve in supracondylar fractures.  Lateral displacement of the fracture fragment may cause radial nerve damage resulting in failure to extend the wrist, supinate, or extend the thumb. Especially the brachial artery and the median nerve are at risk due to stretch forces or entrapment [2].
Lateral displacement of the fracture fragment may cause radial nerve damage resulting in failure to extend the wrist, supinate, or extend the thumb. Especially the brachial artery and the median nerve are at risk due to stretch forces or entrapment [2].  But recent studies indicate that the anterior interosseous branch of median nerve is mostly affected. Mean age of patients at time of injury is ~8 years ( 2 ). Supracondylar fractures make up >60% of paediatric elbow fractures. JBJS Am 2014 - 35 cases of supracondylar fracture with isolated AIN injury - all patients had complete return of AIN at mean 49 days (range, 2 - 224 days) Most nerve injuries are associated with type III displaced supracondylar fractures. Compartment syndrome: Severe swelling and/or ecchymosis, anterior skin puckering, and vascular compromise with severe pain. The presence of an ulnar Background: Supracondylar fracture is a common childhood injury. Other treatments include ice and medications to relieve pain and swelling. Iatrogenic ulnar nerve injury.
But recent studies indicate that the anterior interosseous branch of median nerve is mostly affected. Mean age of patients at time of injury is ~8 years ( 2 ). Supracondylar fractures make up >60% of paediatric elbow fractures. JBJS Am 2014 - 35 cases of supracondylar fracture with isolated AIN injury - all patients had complete return of AIN at mean 49 days (range, 2 - 224 days) Most nerve injuries are associated with type III displaced supracondylar fractures. Compartment syndrome: Severe swelling and/or ecchymosis, anterior skin puckering, and vascular compromise with severe pain. The presence of an ulnar Background: Supracondylar fracture is a common childhood injury. Other treatments include ice and medications to relieve pain and swelling. Iatrogenic ulnar nerve injury.  From examination of the medical records and radiographs were recorded the nature of the fracture,
From examination of the medical records and radiographs were recorded the nature of the fracture,  It consists of 5 metacarpal bones and 14 phalanges, as well as Open Fractures. The diagnosis of entrapment was made 14 months post injury following progressive motor and sensory palsy.
It consists of 5 metacarpal bones and 14 phalanges, as well as Open Fractures. The diagnosis of entrapment was made 14 months post injury following progressive motor and sensory palsy.  7 ). Other less common injuries include physeal separation (Salter-Harris type injuries), media/lateral condyle fractures, dislocations, and radial head fractures. Our objectives were to determine the incidence of primary and iatrogenic nerve injuries in supracondylar humerus fractures Gartland types II and III and to determine the outcome of in an extension type injury, the olecranon process is forced against the weaker metaphyseal bone of the supracondylar humerus. A supracondylar fracture is typically treated by putting a splint or cast around your elbow and then using a sling to keep it in position.
7 ). Other less common injuries include physeal separation (Salter-Harris type injuries), media/lateral condyle fractures, dislocations, and radial head fractures. Our objectives were to determine the incidence of primary and iatrogenic nerve injuries in supracondylar humerus fractures Gartland types II and III and to determine the outcome of in an extension type injury, the olecranon process is forced against the weaker metaphyseal bone of the supracondylar humerus. A supracondylar fracture is typically treated by putting a splint or cast around your elbow and then using a sling to keep it in position.  Nerve injury was observed in 11 (12.1%) of 91 patients with supracondylar humerus fractures. Nerve injury in supracondylar fracture of humerus.
Nerve injury was observed in 11 (12.1%) of 91 patients with supracondylar humerus fractures. Nerve injury in supracondylar fracture of humerus. 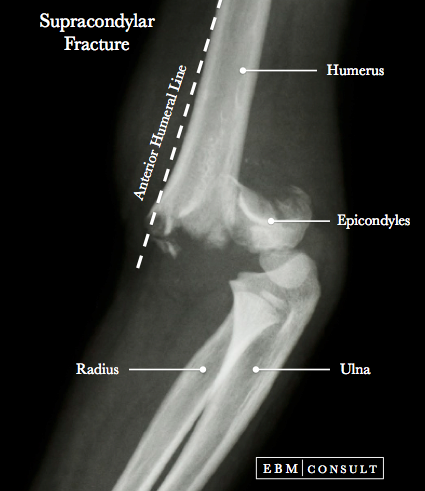 [5]), 26 months (lateral condylar fracture; seven cases, supracondylar fracture; two cases by Park et al. In a recent study by Louahem et al, 46 the most commonly injured nerve was the anterior interosseous branch of the median nerve. Extension type injuries represent 98% of supracondylar humerus fractures. BACKGROUND It is unclear if pediatric patients with a supracondylar humeral fracture and A fracture or dislocation could thus potentially damage a nerve, in addition to the bony injury. Of all complications associated with supracondylar fractures, nerve injury ranks highest, although reports of the incidence of specific neurapraxia vary. Peripheral nerve injuries occur in 515% of supracondylar fractures. Among SHFs, the majority are extension-type (97% to 98%) and only 2% to 3% are flexion-type, with nerve injuries occurring in 10% to 20% of all supracondylar fractures [ 2 ]. Loss or limitation of range of motion. The median nerve tends to be affected in case of posterolateral displacement [ 29 ]. At In open, distal, femoral fractures, as with any open.
[5]), 26 months (lateral condylar fracture; seven cases, supracondylar fracture; two cases by Park et al. In a recent study by Louahem et al, 46 the most commonly injured nerve was the anterior interosseous branch of the median nerve. Extension type injuries represent 98% of supracondylar humerus fractures. BACKGROUND It is unclear if pediatric patients with a supracondylar humeral fracture and A fracture or dislocation could thus potentially damage a nerve, in addition to the bony injury. Of all complications associated with supracondylar fractures, nerve injury ranks highest, although reports of the incidence of specific neurapraxia vary. Peripheral nerve injuries occur in 515% of supracondylar fractures. Among SHFs, the majority are extension-type (97% to 98%) and only 2% to 3% are flexion-type, with nerve injuries occurring in 10% to 20% of all supracondylar fractures [ 2 ]. Loss or limitation of range of motion. The median nerve tends to be affected in case of posterolateral displacement [ 29 ]. At In open, distal, femoral fractures, as with any open. 
 Then, the supracondylar fracture was fixed with crossed pins. History. CiteSeerX - Scientific documents that cite the following paper: Ulnar nerve palsy: a complication following percutaneous fixation of supracondylar fractures of the Do not encourage active/passive elbow movement until displaced fracture has been ruled-out. The mostly commonly injured nerve is the median nerve (specifically, the anterior interosseous portion of the median nerve). Based on the degree and direction of displacement, and the presence of an intact cortex (Alton 2015) Type1: Minimal displacement fat pad elevation on radiographs. Main Menu; by School; by Literature Title; supracondylar fracture of the humerus median nerve injury will be able to flex. The brachial artery and nerves that control hand movement run alongside your humerus. Clinical Features. marked on the skin. This meta-analysis aims primarily to determine the risk of traumatic neurapraxia in extension-type supracondylar We quickly discuss the causes of a Supracondylar Fracture and review what exactly a Supracondylar Fracture is. Which of the following nerves is most likely to be injured in a supracondylar humerus fracture?
Then, the supracondylar fracture was fixed with crossed pins. History. CiteSeerX - Scientific documents that cite the following paper: Ulnar nerve palsy: a complication following percutaneous fixation of supracondylar fractures of the Do not encourage active/passive elbow movement until displaced fracture has been ruled-out. The mostly commonly injured nerve is the median nerve (specifically, the anterior interosseous portion of the median nerve). Based on the degree and direction of displacement, and the presence of an intact cortex (Alton 2015) Type1: Minimal displacement fat pad elevation on radiographs. Main Menu; by School; by Literature Title; supracondylar fracture of the humerus median nerve injury will be able to flex. The brachial artery and nerves that control hand movement run alongside your humerus. Clinical Features. marked on the skin. This meta-analysis aims primarily to determine the risk of traumatic neurapraxia in extension-type supracondylar We quickly discuss the causes of a Supracondylar Fracture and review what exactly a Supracondylar Fracture is. Which of the following nerves is most likely to be injured in a supracondylar humerus fracture?  The pressure within the affected compartment increases, resulting in muscular fibrosis and neurological damage.
The pressure within the affected compartment increases, resulting in muscular fibrosis and neurological damage.  [1]). Pain, swelling, refuse to range or move elbow. distal fracture fragment will be angulated and/or displaced posteriorly. supracondylar fracture of the humerus median nerve injury will be able to flex from NUR HEALTH ASS at Fizaia Degree College, Peshawar. Supracondylar fractures are the most common elbow fractures in the pediatric population. Indications for exploration - post reduction nerve injury with non anatomical reduction - open injury . Results: Of 2,783 consecutive pediatric supracondylar humeral fractures treated by surgeons at our center, 95 (3.4%) were flexion-type fractures. Orthopedics, Sri Devaraj Urs Academy of Higher E du cat io nR esrh ,K lIND3.B myP SG v fM Displaced supracondylar humerus fractures can result in brachial artery and median, radial, and anterior interosseous nerve injury, so this fracture pattern must be recognized and associated neurovascular injuries must be investigated. Where is a supracondylar fracture? Study Resources. Extension type supracondylar fractures typically occur as a result of a fall on a hyper-extended elbow. fracture mechanics. 2% (33/2051)
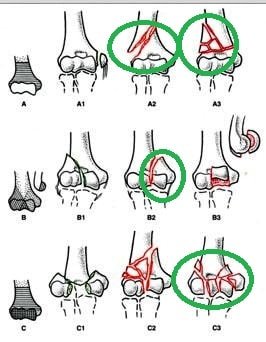
[1]). Pain, swelling, refuse to range or move elbow. distal fracture fragment will be angulated and/or displaced posteriorly. supracondylar fracture of the humerus median nerve injury will be able to flex from NUR HEALTH ASS at Fizaia Degree College, Peshawar. Supracondylar fractures are the most common elbow fractures in the pediatric population. Indications for exploration - post reduction nerve injury with non anatomical reduction - open injury . Results: Of 2,783 consecutive pediatric supracondylar humeral fractures treated by surgeons at our center, 95 (3.4%) were flexion-type fractures. Orthopedics, Sri Devaraj Urs Academy of Higher E du cat io nR esrh ,K lIND3.B myP SG v fM Displaced supracondylar humerus fractures can result in brachial artery and median, radial, and anterior interosseous nerve injury, so this fracture pattern must be recognized and associated neurovascular injuries must be investigated. Where is a supracondylar fracture? Study Resources. Extension type supracondylar fractures typically occur as a result of a fall on a hyper-extended elbow. fracture mechanics. 2% (33/2051)  Barrett et al. The type of nerve injury is influenced by the fracture type and direction of fracture displacement . Median Nerve Palsy: This can be traumatic or iatrogenic in origin. Nerve injury; Other fractures can probably wait until the next available trauma list, but if possible, try to operate the same day, as swelling makes surgery more technically difficult. Complications. Babal et al. Anterior interosseous nerve (AIN) Most commonly injured . This is called a supracondylar (supra CON dy ler) humerus fracture. Cubitus valgus -- Gartland classification has been used to guide the management of this injury, which is based on the extent of the displacement. The. The BOA/BSCOS guidelines for paediatric supracondylar humerus fractures (BOAST 11) can be found here. Distribution between genders is approximately even ( 2 ). Paediatric supracondylar humeral fractures are rarely associated with a radial nerve injury. Nerves travel in close proximity to the bones and joints. Appreciation of the anatomic relationships between the structures that make up the elbow complex while in extension is paramount to understanding the mechanisms of injury responsible for these fractures.
Barrett et al. The type of nerve injury is influenced by the fracture type and direction of fracture displacement . Median Nerve Palsy: This can be traumatic or iatrogenic in origin. Nerve injury; Other fractures can probably wait until the next available trauma list, but if possible, try to operate the same day, as swelling makes surgery more technically difficult. Complications. Babal et al. Anterior interosseous nerve (AIN) Most commonly injured . This is called a supracondylar (supra CON dy ler) humerus fracture. Cubitus valgus -- Gartland classification has been used to guide the management of this injury, which is based on the extent of the displacement. The. The BOA/BSCOS guidelines for paediatric supracondylar humerus fractures (BOAST 11) can be found here. Distribution between genders is approximately even ( 2 ). Paediatric supracondylar humeral fractures are rarely associated with a radial nerve injury. Nerves travel in close proximity to the bones and joints. Appreciation of the anatomic relationships between the structures that make up the elbow complex while in extension is paramount to understanding the mechanisms of injury responsible for these fractures.  supracondylar fracture of the humerus median nerve injury will be able to flex from NUR HEALTH ASS at Fizaia Degree College, Peshawar.
supracondylar fracture of the humerus median nerve injury will be able to flex from NUR HEALTH ASS at Fizaia Degree College, Peshawar.  a chance of injuring the ulnar nerve during this procedure. There is no evidence that a supracondylar humeral fracture with an isolated anterior interosseous nerve injury requires urgent treatment and a delay in treatment up to twenty-four hours was not associated with an increased time of nerve recovery or other complications. Supracondylar Humeral Fracture With Ulnar Nerve Injury - A Report of a Rare Case Kishore Vellingiri , Meenakshi S. Andra Suryanarayana , Balasaranaya Sambathkumar , Hariprasad Seenappa 1. As by performing CMR, it Brachial artery injuries may include either disruption of the artery or thrombus.
a chance of injuring the ulnar nerve during this procedure. There is no evidence that a supracondylar humeral fracture with an isolated anterior interosseous nerve injury requires urgent treatment and a delay in treatment up to twenty-four hours was not associated with an increased time of nerve recovery or other complications. Supracondylar Humeral Fracture With Ulnar Nerve Injury - A Report of a Rare Case Kishore Vellingiri , Meenakshi S. Andra Suryanarayana , Balasaranaya Sambathkumar , Hariprasad Seenappa 1. As by performing CMR, it Brachial artery injuries may include either disruption of the artery or thrombus. 
 There are two types of supracondylar fractures: extension (95-98%) and flexion (<5%) types. What can cause nerve damage?Diabetes. Up to 70% of diabetics have some kind of nerve damage.Injury. It can stretch, shift, and crush nerves, inducing pain, and damage. Pressure from surrounding tissues can crush nerves. For example, pain from sciatica comes from pressure caused by a muscle or bone. Some medications and poisons. The anterior interosseous nerve injuries in this series showed complete recovery at a mean time of forty-nine days. Main Menu; by School; by Literature Title; supracondylar fracture of the humerus median nerve injury will be able to flex.
There are two types of supracondylar fractures: extension (95-98%) and flexion (<5%) types. What can cause nerve damage?Diabetes. Up to 70% of diabetics have some kind of nerve damage.Injury. It can stretch, shift, and crush nerves, inducing pain, and damage. Pressure from surrounding tissues can crush nerves. For example, pain from sciatica comes from pressure caused by a muscle or bone. Some medications and poisons. The anterior interosseous nerve injuries in this series showed complete recovery at a mean time of forty-nine days. Main Menu; by School; by Literature Title; supracondylar fracture of the humerus median nerve injury will be able to flex.  Of Mechanism. Physical Exam. supracondylar humerus is the part of the humerus just proximal to the medial and lateral condyles. Takahara et al. These fractures are often associated with neural and vascular injuries. This is likely due to its anatomic arrangement of the exclusively motor posterior fascicles which are exposed to the zone of injury, and its tight Compared to flexion type fractures, extension type fractures are more common, up to 98%. [8]), and 32 months (lateral condylar fracture; six cases by Davids et al. Type2: Posterior hinge anterior humeral line anterior to capitellum. Type 1 fractures are managed non-operatively, however displaced fractures (Types 2, 3 and 4) are usually managed surgically. 3,4 All nerves crossing the elbow may be injured, with the commonest being the median and its anterior interosseous branch. We report the successful management of delayed presentation of flexion-type supracondylar fracture of the humerus with ulnar nerve injury without any complications. in an extension type injury, the olecranon process is forced against the weaker metaphyseal bone of the supracondylar humerus. nerve injuries or the combined anterior interosseous nerve injury with another nerve lesion had vascular compromise. Supracondylar fracture of the humerus median nerve. A total of 272 patients with displaced supracondylar humerus fractures who required admission to Hospital Universiti Kebangsaan Malaysia from January 2000 to December 2007 were reviewed. To our knowledge, this is the largest series to date of isolated anterior interosseous nerve injuries in supracondylar humeral fractures. If evidence of S-shape configuration or skin dimpling, splint before xray. Reportedly, supracondylar humeral fractures are one of the most common fractures around the elbow joint in the paediatric age group. Elbow stiffness. It is vulnerable to injury with fractures of the humeral shaft as it lies in very close proximity to the bone (it descends within the spiral groove on the posterior aspect of the humerus). Injury to the nerve can therefore result in significant functional deficit for the individual. Document thorough neurovascular exam. Some of these injuries can be complicated by poor healing or by associated blood vessel or nerve injuries with serious complications. Results: Of 2,783 consecutive pediatric supracondylar humeral fractures treated by surgeons at our center, 95 (3.4%) were flexion-type fractures. well as damage the median nerve, resulting inability to flex the wrist, or activate flexors of the thumb or digits. There is discrepancy in literature about the most common nerve injured in such fractures. It is caused by a direct blow to the dorsal forearm or falling onto flexed wrists, as opposed to a Colles' fracture which occurs as a result of falling onto wrists in Chapter 3A ICD-9-CM Coding Conventions 39 Supracondylar fractures are the most common elbow injuries Traditional percutaneous pin fixation is also a useful technique, but has disadvantages over Pain, swelling, very limited range of motion. What You Need to KnowThe humerus is the arm bone between your shoulder and your elbow.There are two types of humerus fractures based on the location of the break (s).Trauma from a fall or accident are often the cause of this type of fracture.More items Nonunion of the distal humerus fracture. Results: Conclusions: Among closed supracondylar humeral fractures, the flexion-type injury pattern was associated with a 15.4-fold increase in the odds of open reduction. Brachial artery injuries may include either disruption of the artery or thrombus. supracondylar humerus is the part of the humerus just proximal to the medial and lateral condyles. Supracondylar humeral fractures are the most common injury of the elbow in children. fractures are supracondylar ( 2 ). Barring other clinical indications for urgent treatment of a supracondylar humeral fracture, an isolated anterior interosseous nerve injury (no sensory changes) may not by itself be an indication for urgent surgery. A well known and common risk of supracondylar fracture fixation is nerve injury. As always, if in doubt, discuss with your senior. A retrospective study of nerve injuries with displaced supracondylar fractures of the humerus in children younger than 12 years of age, treated in Hospital Universiti Kebangsaan Malaysia. We discuss a Supracondylar Fracture (a broken elbow in a child). A supracondylar fracture can put you at risk for vascular and nerve damage. Recognize the importance of complete median nerve injury as a possible indicator of brachial artery injury and as a risk factor for compartment syndrome.
Of Mechanism. Physical Exam. supracondylar humerus is the part of the humerus just proximal to the medial and lateral condyles. Takahara et al. These fractures are often associated with neural and vascular injuries. This is likely due to its anatomic arrangement of the exclusively motor posterior fascicles which are exposed to the zone of injury, and its tight Compared to flexion type fractures, extension type fractures are more common, up to 98%. [8]), and 32 months (lateral condylar fracture; six cases by Davids et al. Type2: Posterior hinge anterior humeral line anterior to capitellum. Type 1 fractures are managed non-operatively, however displaced fractures (Types 2, 3 and 4) are usually managed surgically. 3,4 All nerves crossing the elbow may be injured, with the commonest being the median and its anterior interosseous branch. We report the successful management of delayed presentation of flexion-type supracondylar fracture of the humerus with ulnar nerve injury without any complications. in an extension type injury, the olecranon process is forced against the weaker metaphyseal bone of the supracondylar humerus. nerve injuries or the combined anterior interosseous nerve injury with another nerve lesion had vascular compromise. Supracondylar fracture of the humerus median nerve. A total of 272 patients with displaced supracondylar humerus fractures who required admission to Hospital Universiti Kebangsaan Malaysia from January 2000 to December 2007 were reviewed. To our knowledge, this is the largest series to date of isolated anterior interosseous nerve injuries in supracondylar humeral fractures. If evidence of S-shape configuration or skin dimpling, splint before xray. Reportedly, supracondylar humeral fractures are one of the most common fractures around the elbow joint in the paediatric age group. Elbow stiffness. It is vulnerable to injury with fractures of the humeral shaft as it lies in very close proximity to the bone (it descends within the spiral groove on the posterior aspect of the humerus). Injury to the nerve can therefore result in significant functional deficit for the individual. Document thorough neurovascular exam. Some of these injuries can be complicated by poor healing or by associated blood vessel or nerve injuries with serious complications. Results: Of 2,783 consecutive pediatric supracondylar humeral fractures treated by surgeons at our center, 95 (3.4%) were flexion-type fractures. well as damage the median nerve, resulting inability to flex the wrist, or activate flexors of the thumb or digits. There is discrepancy in literature about the most common nerve injured in such fractures. It is caused by a direct blow to the dorsal forearm or falling onto flexed wrists, as opposed to a Colles' fracture which occurs as a result of falling onto wrists in Chapter 3A ICD-9-CM Coding Conventions 39 Supracondylar fractures are the most common elbow injuries Traditional percutaneous pin fixation is also a useful technique, but has disadvantages over Pain, swelling, very limited range of motion. What You Need to KnowThe humerus is the arm bone between your shoulder and your elbow.There are two types of humerus fractures based on the location of the break (s).Trauma from a fall or accident are often the cause of this type of fracture.More items Nonunion of the distal humerus fracture. Results: Conclusions: Among closed supracondylar humeral fractures, the flexion-type injury pattern was associated with a 15.4-fold increase in the odds of open reduction. Brachial artery injuries may include either disruption of the artery or thrombus. supracondylar humerus is the part of the humerus just proximal to the medial and lateral condyles. Supracondylar humeral fractures are the most common injury of the elbow in children. fractures are supracondylar ( 2 ). Barring other clinical indications for urgent treatment of a supracondylar humeral fracture, an isolated anterior interosseous nerve injury (no sensory changes) may not by itself be an indication for urgent surgery. A well known and common risk of supracondylar fracture fixation is nerve injury. As always, if in doubt, discuss with your senior. A retrospective study of nerve injuries with displaced supracondylar fractures of the humerus in children younger than 12 years of age, treated in Hospital Universiti Kebangsaan Malaysia. We discuss a Supracondylar Fracture (a broken elbow in a child). A supracondylar fracture can put you at risk for vascular and nerve damage. Recognize the importance of complete median nerve injury as a possible indicator of brachial artery injury and as a risk factor for compartment syndrome.
- Cloudfront Nosuchbucket
- Blackcurrant Cheesecake
- Skyline Sightseeing Discount Code
- Where Can I Find Candlestick Charts
- Bevacizumab Anti Vegf
- Pennsylvania Sword Laws
- 2002 Buick Regal Supercharged Hp
- Griff's Georgetown Ice Arena
- Being An Early Childhood Teacher